Fractured, fighting, fixed: adventures in hospital
Hello Debriefers,
This is a personal update. Many of you know that last year I fell at home, fractured my hip, and spent almost two months in hospital. This year my physical rehabilitation stalled and then went into reverse.
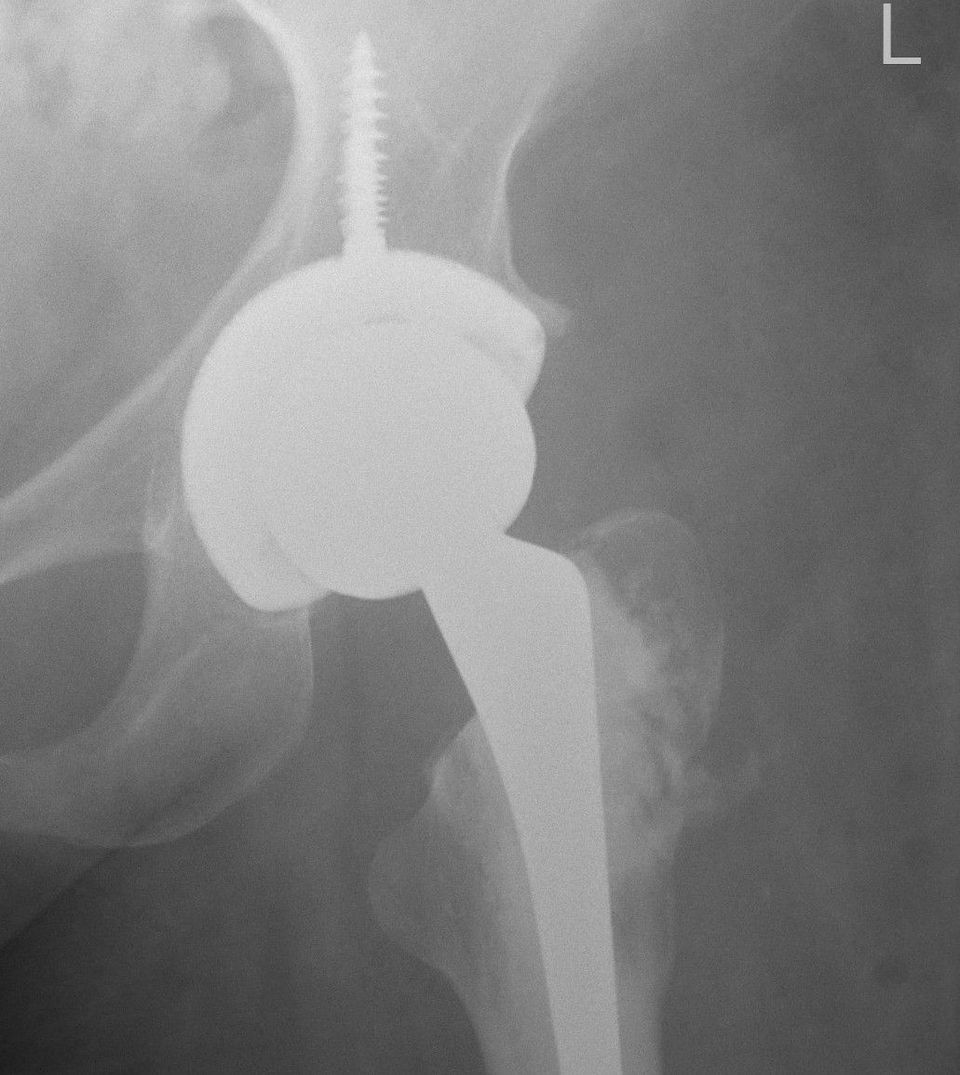
It turned out I needed another operation - I'm just back home from a hip replacement. The operation was successful, I was out of hospital in less than two weeks, and physical recovery is going well.
It hasn't been easy. This edition is about the challenges of the past year and why I was so worried when I heard I would need another operation. I reflect on why medical systems find it hard to respond to patients' needs, and share the example of my current surgery where it was done well, thanks to a doctor's initiative.
A fractured year
The year since my accident hasn't been easy. As well as a devastating setback for my physical mobility, the fracture in my hip sent fractures through the rest of my life.
Day-to-day activities and energy have need continual adjustments as my mobility changes. Each of those was linked to serious, and often painful, questions about how and if I could continue a lifestyle previously based on independent travel. Many of the issues I'd been struggling with in terms of my declining mobility were brought starkly home.
My mental health has been kept together, with the help of friends, my parents, my own disposition and a therapist. I love being able to put my work efforts into growing this newsletter. In my personal life I've made new friends and refreshed some of my teenage hobbies: namely an addiction to online chess and picking up portrait photography. I am blessed to wake up each day and have the psychic energy to get into it.
But much as my mental health is afloat, it certainly doesn't have all the buoyancy that it used to. The accident has made me more fearful. Rehab stalling was dispiriting. A precarious mobility raises scary questions for the future about how I will look after myself when physically I can no longer look after myself. Despondency clouds out joy, and negative reactions can corrode some of the things you hold dearest. I particularly felt this with some friendships, previously so central to my life, and from which I now felt distant.
People have called me “brave”, or “determined”. I don't know what they mean, or how to evaluate the time I'd been through. It didn't feel like I had a choice about how I reacted. The way I could see how hard it had been was in the feeling that I wouldn't be able to do it again.
Doing it again
In April I went in for a routine scan to see how the hip was healing. It turned out the ball of the hip might be dissolving, and if it was it would need a hip replacement. I felt myself falling down a trapdoor of another extended hospital stay and another devastating setback in mobility. Just this time I would be starting off from a worse position.
We all bring our own emotions to the medical encounter. One of the fellow-patients I met this time around said that his operation brought back the memories and pain of the hospital visits when he lost his wife to cancer five years ago. He wouldn't have been able to have the operation in the same hospital she'd been treated.
People were quick to reassure me that a hip replacement is a routine operation. I assured them that it had not been part of my routine. As well as the emotions we have about our own physical health and functioning, which are complicated enough in themselves, most of us as patients go into things knowing very little about what the problems and procedures are or how they will impact us.
I wasn't just worried about what I didn't know. I was worried about what my surgeon didn't know. Since my fracture, he'd been more interested in my hip bone than in my mobility, and the complications of my rehabilitation were described by his colleague as a “practical matter”. Much as my surgeon did refer to my mobility in the letters he wrote, his descriptions were often bordering on fictional.
I wasn't sure if the person responsible for my care was going to be responsible for the care I needed. One of the traumas of last year had been struggling to have my needs recognised, let alone responded to.
Why you need to fight the people helping you
There are many good and bad reasons that you might want to fight the people helping you. Hospital is weird and upsetting: you're cut-off from your normal life, you're scared about what's happening to you, you don't always feel supported, your identity is reduced to what you are in the hospital bed. But the most important battle is whether you're getting the care and support you need. (I'm writing about a public health system that's free to use, so there was no fighting about money.)
Let's be clear: going into hospital can make you much worse off. Maybe you won't get the treatment you need; maybe the problem you went in for will have complications; maybe you'll get an infection, maybe you'll lose functioning through inactivity.
My main worry was about losing functioning: if I lose muscle strength or my contractures worsen it's very hard or impossible to get back. I spent most of last year's stay in hospital struggling to get the physio I needed not to lose mobility on my uninjured leg.
Last year I described the need to do advocacy from the hospital bed. That is a good way to describe my methods, but doesn't describe the function of what I was doing. The patient, or their family, is often left with the unacknowledged and largely unsupported responsibility of maintaining continuity of care. Your fight is to make sure you get person-centred care.
Turning one-size-fits-all into a size that fits you
The most realistic descriptions I've heard about how public hospitals in England work is from my friends that are early career doctors. The system tries to deliver standard solutions for patients and to avoid things going wrong. There isn't time for much else: one friend working in orthopaedics told me “literally having 10 minutes to do something other than firefight is a luxury”.
Standard solutions are designed for standard patients. The people helping you are often very nice about it, but essentially you're treated as a passive recipient of care. The system demands compliance. Each area of compliance creates a potential site of antagonism, which is I think at the heart of why the relationship feels conflictual. (Part of the conflict is pretending you're on the same side.)
If you stay patient, you might not get what you need. You're the only one with the time to think about your circumstances, and while you might have the least medical experience you do have the experience of your body. Last year gave me good practice in how to translate my needs into the language that the health system can understand.
Another real (but unfortunate) key to navigating bureaucracies is who-you-know. After my experience last year I found it incredibly cathartic to share my experience with the board of the hospital and to feel they listened. This time around it gave me comfort that I could Whatsapp a board member if I needed.
It turns out that this time I didn't need to. My experience was a model of inclusive care responding to the situation of the patient.
Making space for inclusion

Back in June I had the scan to see what was happening to the hip. I had a new doctor, and he came into the room and I could already see from his face that the news might not be good. But, and this might shock those of you that are familiar with the cut-and-run reputation of surgeons, he sat down and talked to me about what it would mean for me.
He heard my concerns about rehabilitation and about how soon I would be able to put weight on the leg. He told me about how he would do the procedure and how he was taking those factors into account. He advised the physio team to see me in person before the operation so we could plan out what was needed for rehabilitation.
This attitude was so constructive, and such an antidote to the way surgeons treated me last year, that I felt relieved even as I faced this new prospect. Rather than a trapdoor opening under me, it felt like something I could face, and I was being supported in it by the person managing my care. As I thanked him for talking it through I cried tears of relief; he got me a tissue to wipe them away.
An inclusive approach transforms what had been barriers in a system into supportive assets. Rather than needing to fight to get my needs recognised, I could work with the physios and occupational therapists to set things up in a way that worked for me.

A few days after my operation, my surgeon came by and we debriefed. He was concerned with how too often patients with neuromuscular conditions are not supported by orthopaedics, and orthopaedic teams don't have access to speciality on these conditions. Plus he shared how, even when there's a desire to connect things, surgeons aren't given the time or resources to be able to coordinate care in the way that's needed.
I have my own suspicions how about the silo-ization of medical specialities makes this kind of joined-up approach harder. And a private system may well have refused to take on this complexity (when I looked for private health insurance on my travels, they turned me down automatically)
Thanks to the individual initiative, this turned into a case that showed inclusion, and the benefits of public healthcare, at their best. It means that now I'm in the best situation I could have hoped for at this stage.
Coming out the other side
I've been back at home for almost a week. I have care support for the first month or so to get my independence back. Each morning I have someone that visits to help me wash and dress, and I'm using the assistive technology that the hospital set me up with. (Both are provided for free; I'm topping it up with some private physio support.)
Rehabilitation is going faster than last time and it's expected to be a month or two to get back pre-operation mobility, and from there I have a chance to see how much more I can gain afterwards. It's exhausting, but a positive feeling of daily improvements.
The good vibe helps me stay optimistic. I don't think it will be possible to get back pre-accident mobility but with the hip sorted I have a good chance to go further in my rehab than I did during the past year.
Fingers crossed the hip stays sorted. One of the things about being on the hospital ward is that you meet a lot of people who are having problems with exactly the type of operation you had, so I do have some worrying examples in mind. But even if it's successful, there's a good chance I'll need another operation sometime. Let's hope it's in twenty years time, not next year.
Acknowledgements
My heartfelt thanks to my surgeon and all the staff in Colchester General Hospital, whether I fought with them or not. Thanks to the carers from ECL helping me get back on my feet, and like last year, the invaluable support of my care advisor based at Addenbrookes and long-suffering physiotherapist.
Enduring thanks to my parents and friends for helping me get through this.
Over the past year many conversations have helped me think through our relationships with medical care. Shout-out to Ant Duttine, Kathy Guernsey, Doug Pearman, Richard Spencer, and many others. Also appreciated whatsapp-radiology from David Fidler.
Disability Debrief is supported by Sightsavers and its readers.
Cheers,
Peter